Overview
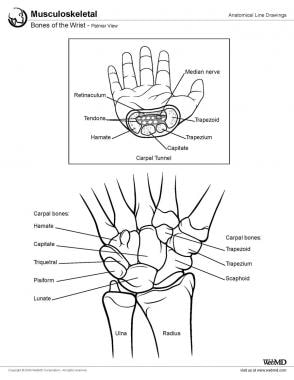
The wrist is a complex joint that bridges the hand to the forearm. It is actually a collection of multiple bones and joints. The bones comprising the wrist include the distal ends of the radius and ulna, 8 carpal bones, and the proximal portions of the 5 metacarpal bones (see the images below).

All of these bones participate in complex articulations that allow variable mobility of the hand. Relative to the forearm, the hand is capable of 3 degrees of freedom: (1) flexing and extending, (2) pronating and supinating, and (3) deviating ulnarly or radially. [1, 6, 7, 8, 9] In order to maintain mobility without sacrificing stability, the wrist joint has a complex configuration of ligaments, as shown in the following images.
Gross Anatomy
The anatomic linkage between the distal forearm and the hand is composed of 15 bones: 8 carpal bones, the distal radius and ulnar, and the bases of the 5 metacarpals.
Carpal bones
The carpal bones are organized into 2 groups, a proximal row and a distal row. The proximal row is found at the level of the distal wrist crease and includes the scaphoid, lunate, triquetrum, and pisiform. The second row of carpal bones, the distal row, is made up of the trapezium, trapezoid, capitate, and hamate; the distal row articulates with the bases of the 5 metacarpal bones. The proximal carpal row bones represent an intercalated segment, as no tendons insert upon them. [10] For this reason, their movement is dependent entirely on mechanical forces from surrounding articulations.
The bones of the distal row are closely adherent to each other via intercarpal ligaments (see the images below). These bones are also tightly bound to the metacarpal bones, representing the carpometacarpal (CMC) joint. In particular, the ligamentous connection between the trapezoid and capitate to the index (second) and middle (third) finger metacarpals, respectively, are so rigid that the distal carpal row has been considered a component of a fixed hand unit that moves in response to musculotendinous forces generated from the forearm. [11]
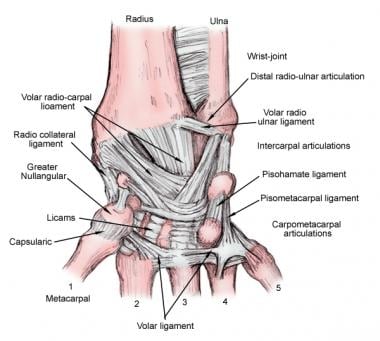
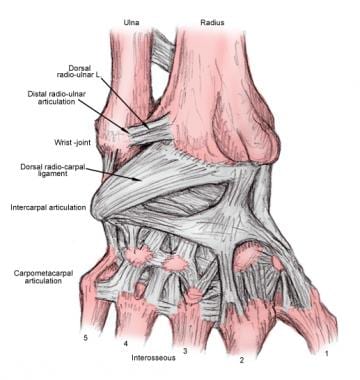
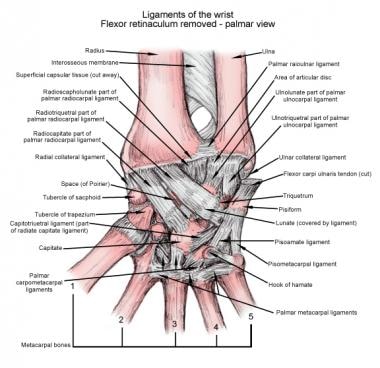
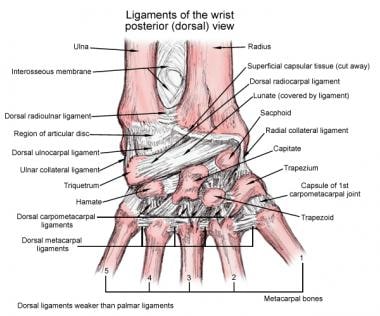
The joints of the wrist are surrounded by a fibrous capsule and are held together by an array of ligaments that provide carpal stability by linking the bones both dorsally and volarly (see the following images). These carpal ligaments are divided into 2 groups: intrinsic ligaments that originate and insert on carpal bones and extrinsic ligaments that bridge carpal bones to the radius or metacarpals. [12]
Extrinsic ligaments, volar
Radioscaphocapitate ligament
Located ulnar to the radial collateral ligament, the radioscaphocapitate ligament originates from the radial styloid process, passes beneath the waist of the scaphoid, and inserts onto the capitate, creating a sling to support the scaphoid. [1]
Long radiolunate ligament
The long radiolunate ligament originates at the distal radius from the volar aspect of scaphoid fossa. The proximal attachment is partially overlapped by the radioscaphocapitate ligament. It inserts radially on the distal surface of the lunate as well as the volar segment of the scapholunate interosseous ligament without directly attaching to the scaphoid. The long radiolunate ligament provides stability to counteract ulnar or distal translocation of the lunate. The space of Poirier represents an area of weakness between the long radiolunate and radioscaphocapitate ligaments at the level of the midcarpal joint. [1]
Short radiolunate ligament
The short radiolunate ligament originates at the distal radius on the ulnar and volar edge of the lunate fossa and inserts into the volar aspect of the lunate. Its insertion is located proximal to the insertion of the ulnolunate ligament. The short radiolunate ligament has a potential role in lunate stabilization. [1, 13]
Radioscapholunate ligament
The radioscapholunate ligament is found between the long and short radiolunate ligaments at the distal radius in the region spanning the scaphoid and lunate fossa. The radioscapholunate ligament attaches distally between the volar and proximal segments of the scapholunate interosseous ligament at both the scaphoid and lunate.
This ligament is not considered a true ligament, because it is composed of vascular and neural elements and no ligamentous tissue. [13] For this reason, it does not add any substantial mechanical support. [1]
Ulnolunate ligament
The ulnolunate ligament's origin is radial to the ulnocapitate ligament at the base of the ulnar styloid process. Distally, it inserts on the ulnar side of the lunate, distal to the insertion of the short radiolunate ligament. [1]
Ulnocapitate ligament
The ulnocapitate ligament is proximally attached at the fovea of the ulnar head, with its insertion distally attached onto the proximal and volar region of capitiate (see the image below). [1]
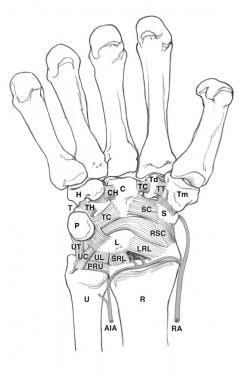 Volar carpal ligaments and bones. AIA = anterior interosseous artery; C = capitate; CH = capitohamate; H = hamate; L= lunate; LRL = long radiolunate ligament; P = pisiform; PRU = palmar radioulnar ligament; R = radius; RA = radial artery; RSC = radioscapholunate ligament; S = scaphoid; SC = scaphocapitate ligament; SRL = short radiolunate ligament; T = triquetrum; TC = triquetrocapitate ligament; Td = trapezoid; TH = triquetrohamate ligament; Tm = trapezium; TT = trapeziotrapezoid ligament; U = ulna; UC = ulnocarpal ligament; UL = ulnolunate ligament; UT = ulnotriquetral ligament.
Volar carpal ligaments and bones. AIA = anterior interosseous artery; C = capitate; CH = capitohamate; H = hamate; L= lunate; LRL = long radiolunate ligament; P = pisiform; PRU = palmar radioulnar ligament; R = radius; RA = radial artery; RSC = radioscapholunate ligament; S = scaphoid; SC = scaphocapitate ligament; SRL = short radiolunate ligament; T = triquetrum; TC = triquetrocapitate ligament; Td = trapezoid; TH = triquetrohamate ligament; Tm = trapezium; TT = trapeziotrapezoid ligament; U = ulna; UC = ulnocarpal ligament; UL = ulnolunate ligament; UT = ulnotriquetral ligament.
Extrinsic ligaments, dorsal
Intercarpal ligaments
The intercarpal ligaments are secondary stabilizers of the scapholunate joint. [1]
Radiocarpal ligament
The radiocarpal ligament originates from the ulnar and dorsal portion of distal radius between the dorsal radial (Lister) tubercle and the ridge between the scaphoid and lunate fossa. It inserts distally onto the proximal and dorsal tubercles of the triquetrum and the lunate. [1]
Intrinsic ligaments, volar
Lunotriquetral ligament
The lunotriquetral ligament originates from ulnar side of the lunate and attaches to the triquetrum distal to the attachment of the ulnolunate ligament and radial to the lunotriquetral interosseous ligament. [1]
Trapeziotrapezoid ligament
The trapeziotrapezoid ligament attaches to the ulnar aspect of the trapezium and passes ulnarly to the radial edge of the trapezoid. [1]
Scaphotrapezial ligament
Composed of 2 branches, a radial branch and an ulnar branch, both branches of the scaphotrapezial ligament are attached to the radial and volar aspect of the scaphoid tuberosity. The 2 branches travel distally and diverge, forming a V shape. The radial branch attaches to the radial aspect of the trapezium, whereas the ulnar branch attaches to the proximal side. [1]
Scaphotrapezoidal ligament
Along with the scaphotrapezial ligament, the scaphotrapezoidal ligament supports the scaphotrapeziotrapezoidal joint. It attaches to the distal and volar aspect of the scaphoid tuberosity and inserts distally onto the proximal edge of the trapezoid. [1]
Scaphocapitate ligament
The scaphocapitate ligament attaches radially to the ulnar and volar side of the distal pole of the scaphoid and ulnarly to the radial and volar aspect of the capitate. [1]
Capitotrapezoid ligament
The capitotrapezoid ligament originates on the ulnar and volar side of the trapezium and spans the trapezoid to attach to the radial and volar aspect of the capitate. [1]
Capitohamate ligament
The capitohamate ligament attaches to the ulnar region of the capitate and travels ulnarly to the radial edge of the hamate. [1]
Triquetrocapitate ligament
The triquetrocapitate ligament attaches proximal to the volar and radial edge of the triquetrum and inserts distal to the ulnar and volar edge of the capitate. [1]
Triquetrohamate ligament
The triquetrohamate ligament proximally attaches to the distal edge of the triquetrum and distally to the dorsal edge of hamate. Three types of relationships exist between the triquetrocapitate and triquetrohamate ligaments, as follows:
-
Type A: The triquetrocapitate ligament is separate from the triquetrohamate ligament
-
Type B: The triquetrocapitate ligament overlaps the triquetrohamate ligament
-
Type C: The triquetrocapitate ligament has an additional ligament from the triquetrum to the proximal pole of the hamate
Intrinsic ligaments, dorsal
Intercarpal ligament
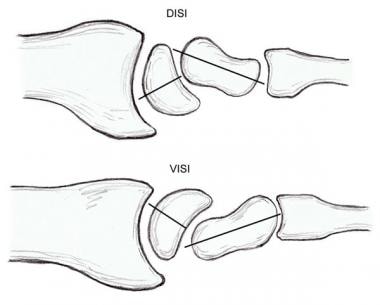
The intercarpal ligament overlaps the dorsal portion of the scapholunate interosseous ligament, with its origin being the distal and radial aspect of the dorsal tubercle of the triquetrum. A lateral "V" configuration with the apex toward the triquetrum is formed by the dorsal intercarpal and dorsal radiocarpal ligaments, providing indirect dorsal stability to the scapholunate complex during wrist motion. [14] Along with the radiocarpal ligament, the intercarpal ligament maintains carpal stability and alignment while preventing dorsal intercalated segment instability (DISI) and volar intercalated segment instability (VISI) deformities. [1]
Trapeziotrapezoid ligament
The trapeziotrapezoid ligament is found at the ulnar edge of the trapezium and travels ulnarly the radial edge of the trapezoid. [1]
Capitotrapezoid ligament
The capitotrapezoid ligament is attached to the ulnar edge of the trapezoid and passes ulnarly to the distal and radial aspect of the capitate. [1]
Capitohamate ligament
Composed of distal and proximal ligaments, the distal component of the capitohamate ligament originates on the distal side of the ulnar edge of the capitate and attaches to the distal side of the radial edge of the hamate. The proximal ligament originates on the ulnar edge of the capitate and attaches to the proximal side of radial edge of the hamate. [1]
Triquetrohamate ligament
Attached proximally to the distal and radial edge of triquetrum, the triquetrohamate ligament inserts distally to the proximal and volar edge of the hamate. [1]
Interosseous ligaments
Scapholunate ligament
The scapholunate ligament connects the scaphoid and lunate along the proximal joint surface and is the primary stabilizer of the scapholunate articulation. It is composed of 3 structures: (1) a volar portion, (2) a dorsal portion, and (3) a proximal portion. The dorsal portion is the thickest of the 3 structures and the most critical of the scapholunate joint stabilizers. [15, 16] Disruption of the ligament allows the lunate to extend when the scaphoid is flexed, creating a dorsal intercalated segment instability (DISI) deformity (see the image below). [1, 17]
Lunotriquetral ligament
The lunotriquetral ligament attaches the lunate and triquetrum along the proximal joint surface. Similar to the scapholunate interosseous joint, this ligament is described as having 3 distinct structures: (1) a volar portion, (2) a dorsal portion, and (3) a proximal portion. Injury to the lunotriquetral ligament permits lunate flexion with a normally aligned scaphoid, creating a volar intercalated segment instability (VISI) deformity (see the image above). [1, 17]
Trapeziotrapezoid ligament
The trapeziotrapezoid ligament joins the trapezium and trapezoid. It is found entirely within the trapeziotrapezoid joint, attaches to the volar side of the ulnar aspect of the trapezium, and travels ulnarly to the distal radial edge of the trapezoid. [1]
Capitotrapezoid ligament
Like the trapeziotrapezoid interosseous ligament, the capitotrapezoid ligament is found within the joint space. It attaches the capitate to the trapezoid. This ligament travels from the central region of the ulnar side of the trapezoid to the distal, radial side of the capitate. [1]
Capitohamate ligament
The capitohamate ligament passes from the center of the ulnar side of the capitate into the radial side of the hamate. This ligament is found entirely within the joint. [1]
Natural Variants
Research over the past few decades has increased our understanding of the normal anatomic variants germane to the hand and wrist. Without this working knowledge, variations in skeletal morphology may be misinterpreted as being clinically abnormal and lead to misdiagnosis and inappropriate intervention.
Carpometacarpal joint
One variation is related to the carpometacarpal joint, more specifically the shape of the fourth metacarpal base. Studies have revealed that the most common variation in the carpometacarpal joint exists at the fourth carpometacarpal joint. The fourth metacarpal base has 5 distinct shapes, categorized as types I-V, as follows:
-
Type I: Broad base with articulation with the hamate and one dorsal facet that is in contact with the capitate
-
Type II: Broad base with articulation with the hamate and 2 facets (dorsal and volar) that articulate with the capitate
-
Type III: Narrow base that solely articulates with the hamate
-
Type IV: Broad base that articulates with the hamate and a single, separate facet that articulates with the capitate
-
Type V: Relatively broad base without any projections or separate articular surface articulates with the hamate and the capitate
Midcarpal joint
In the midcarpal joint, 2 areas of variability have been identified. The first is in relation to the lunate bone. The lunate has variation in relation to the onset of ossification and shape. Ossification in males occurs between ages 1.5 and 7 years and between ages 1 and 6 years in females. Double ossification centers, as well as complete absence of the lunate, have been reported. Two types of lunates have been described; Type I lacks a medial facet, whereas type II has a medial facet that articulates with the hamate. [2]
Another area of variability within the midcarpal joint exists at the distal articulation of the scaphoid. Three variations have been identified: (1) separate facets for articulation with the trapezoid and trapezium, with an interfacet ridge separating the facets; (2) separate trapezoid and trapezium facets with palpable interfacet ridge, not visually identifiable; and (3) smooth articular surface not visually identifiable.
Isolated carpal coalition
Isolated carpal coalition is an anatomic variant with a prevalence of 0.1%. This finding is more common in the black population, commonly bilateral, and has a strong female predilection. The lunotriquetral, followed by the capitohamate, are the most common carpal coalitions. Of note, persons with lunotriquetral coalition may have a widened scapholunate joint, representing a normal variant.
-
Bones of the wrist, palmar view.
-
Bones of the wrist, enlarged view.
-
Cross-section of the wrist joint.
-
Ligaments of the wrist, dorsal view.
-
Volar carpal ligaments.
-
Ligaments of the wrist, palmar view.
-
Ligaments of the wrist, posterior (dorsal) view.
-
Volar carpal ligaments and bones. AIA = anterior interosseous artery; C = capitate; CH = capitohamate; H = hamate; L= lunate; LRL = long radiolunate ligament; P = pisiform; PRU = palmar radioulnar ligament; R = radius; RA = radial artery; RSC = radioscapholunate ligament; S = scaphoid; SC = scaphocapitate ligament; SRL = short radiolunate ligament; T = triquetrum; TC = triquetrocapitate ligament; Td = trapezoid; TH = triquetrohamate ligament; Tm = trapezium; TT = trapeziotrapezoid ligament; U = ulna; UC = ulnocarpal ligament; UL = ulnolunate ligament; UT = ulnotriquetral ligament.
-
Dorsal/volar intercalated segmental instability (DISI/VISI).



